In the last post in this series taken from the 21st G. Gayle Stephens lecture (Family Medicine in the era of health reform - 2, May 11, 2011), I discussed medical student interest in entering family medicine, and in particular a medical student named Kate Dewar featured in a NY Times article (More Physicians Say No to Endless Workdays). Her father and grandfather are primary care physicians but she is entering emergency medicine residency. In this final post, I continue the discussion, looking at changes in primary care practice and its implications for health and health care in the US.
The entire talk, "Family Medicine in the Era of Health Reform", is available at https://docs.google.com/document/d/1bmKCAUljtVgYjyJdStg96IpmajZPTkjCVG1lWtVTxo4/edit?hl=en_US#, in both GoogleDocs (for Chrome or Firefox) and Word (for IE) formats.
Of course, there are changes to primary care practice, but in my opinion, they are not all good. According the NY Times article, for Kate’s father, William Dewar III, “…the burden of trying to be all things to all of his patients became unmanageable. In 2006, after Wayne Memorial Hospital hired hospitalists — doctors who specialize in taking care of hospitalized patients — Dr. Dewar finally gave up hospital rounds. For his hospitalized patients, the change meant putting their trust in a doctor who knew them less intimately but was more available and more adept at hospital care. ‘My patients are getting better care now in the hospital,’ Dr. Dewar said. And the change saved him hours of work each week. ‘It meant getting off the hamster wheel,’ he said.”
Maybe they are getting better care, or maybe he just hopes that they are. And better in what way? It may be that hospitalists, who I call the “4-day ED docs”, are great at technical management but not so good (because of their role; I am not impugning their skill sets) at continuity. When your patient has a cold, or needs a BP check, they may be happy to see your partner, or even go to an urgent care center. But when they are sick enough to need to be in the hospital, when they need someone who knows them, they are not getting it. Yes, maybe they are getting someone who can balance their electrolytes, or operate on them in a skilful manner. Maybe, especially if they are lucky enough to be admitted on a Monday and not a Thursday they will even have a consistent management plan from their hospitalist (if not, perhaps, their nocturnist!) But where is the doctor who knows about them?
The surgeon may operate on your cancer, the oncologist and radiation oncologist may prescribe their treatments, the nephrologist may come in to manage the renal failure from the chemotherapy – but you still need the doctor who knows you. This is not a “social rounds” visit; this is caring for the patient, managing the various specialists. My sister was admitted to a hospitalist service in California some years ago (she is OK now) and after a few days the second (or maybe third) hospitalist told her that she looked a lot better. He’d known her for two days. My other sister, visiting from out of town, said “She may look better to you but she is NOTHING like she was last week! She is in no way back to normal!” Good for sisters who come in from out of town, but what if you don’t have one?
We need more primary care doctors, more family physicians, more doctors who can provide continuity for the health-related portions of our journeys through life. But when we get these doctors, what is their life like? I recently met a very smart and committed young family doctor who works at a Federally Qualified Health Center (FQHC) in one of our more “desirable” cities. Even though she doesn’t deliver babies, and doesn’t take care of patients in the hospital, she still felt she was on a hamster wheel, often giving less-than-the-best-care-she-knew-she-could-give to the patients hustled through so that the FQHC could “make its numbers”. She wanted to know what could be done to support the family doctors who are out there working as hard as they can for relatively little money and in danger of burning out. Apparently, just expanding FQHCs to see more patients is not going to do it.
There has to be a solution that provides the benefits of a primary-care based health system to our people without balancing it on the backs of the primary care doctors, who don’t have enough time with their families and don’t have enough time with their patients. Who have to give up even the satisfactions that come from the happy moments of primary care, like delivering babies, and the times when your patients, admitted to the hospital, really need you. And doing it for a salary that, even if it far exceeds that of the average American, is a fraction of what your medical school classmates are getting for working less hard, and makes it difficult to pay off your loans.
If the US is going to benefit from a primary-care-based health system, it is going to have to address the input and process variables of medical education, that is who is admitted and what their experiences are in medical school, the things that lead them to choose specialties, and also the output variables, what the practice life experience is, and make sure that it is tolerable and sustainable.
We know what the characteristics of medical school applicants who are more likely to enter primary care and rural practice are; dozens of pilot programs have demonstrated them. They are students who are from rural areas, from under-represented minority groups; students who are older, and students who are from lower-income families. They also, on the whole, have lower Medical College Admissions Test (MCAT) scores. For those students who do come from higher-income, white, suburban families (who have always been and continue to be the vast majority of those admitted to medical school), the characteristics are a demonstrated history of service (e.g., Peace Corps, VISTA, Teach for America, carrying the rape crisis pager in college, volunteering in a free clinic).
And we are not, not in large enough numbers, not high enough percents. Demonstration projects are of little use if that is where they stay, if we don’t learn the lessons and implement them for the vast majority of medical school admissions.
The 2010 “Top 25” Family Medicine schools as rated (entirely by survey reputation) by US News vary widely in their percentage and number of students entering primary care. Over the 5 year period 2004-08, they ranged from the University of Minnesota with an average of 17.36% of their class, or 37.8 students, entering FM, to Duke with an average of 2.8% or 3.45 students. Of course, US News’ top 25 are not the same as the actual top 25 in students entering family medicine; my school, the University of Kansas (which is not in the US News’ top 25) averaged 20.3%, or 33.4 students, over that period. Since the national average over that period was 8.71%, or 10.8 students, apparently you can be a top FM school, at least according to US News’, and be well below the national average of students entering FM.
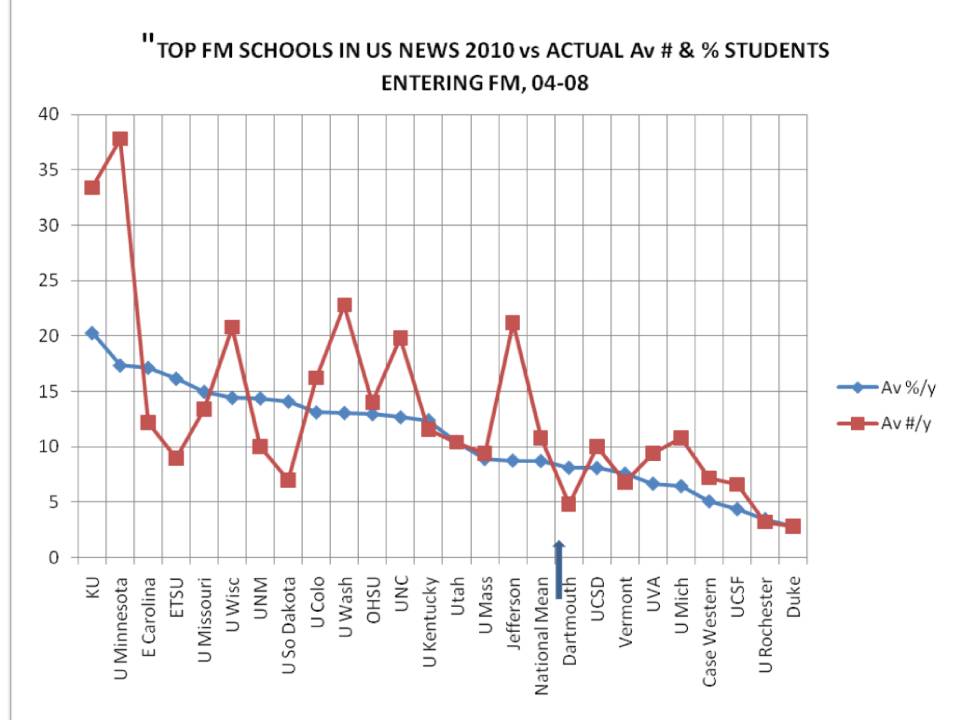
More important, even the actual top schools in producing family doctors have pretty low percentages, ranging from 13% to 20%. We are never going to get to the 40-50% primary care work force we need by producing less than 20% family doctors in the best schools. The worst schools – like Duke, Johns Hopkins and Harvard should be at 20%; KU and Minnesota should be much higher.
And when students are in medical school, we need to be sure both that there is adequate exposure to longitudinal continuity and interdisciplinary and inter-professional primary care, and that those experiences are positive. While I have said that Family Physicians need to be involved in caring for their patients in the hospital, students should not be able to go through medical school, as they do now, thinking that the hospital is the main venue for real health care.
And when those students we have carefully selected and nurtured graduate, and do enter primary care, they need to be able to expect to have reasonable lives. It seems obvious, but a lot of this is about money. Primary care doctors need to make more money, if not in absolute dollars, at least in terms of the percent of subspecialist income. Income does not have to be equal; work from the Robert Graham Center demonstrates that the effect of debt income disappears when primary care doctors make 70% of what specialists make. Medical school debt should be gradually forgiven for students who enter primary care, and forgiven at a much faster rate if they work in a rural area or HPSA.
Where will this money come from? There is no reason to expect that, in a country that already spends twice as much per capita as most other industrialized countries, all of which have better health outcomes, that there will be more money coming into the system. It is going to have to come from other parts of the health sector; the parts being collected now by hospitals and other specialists, in particular. It will also have to come from the profit being taken out of the system by those hospitals and even more by for-profit insurance companies and drug companies. There can be no room for so many “health dollars” going to investor profits, nor can there be perverse financial incentives that make it more desirable to treat sick people than to keep them from getting that sick. There must be a comprehensive approach, for otherwise there will always be “gaming of the system”, and this is where the big failing of ACA is.
We need continue to need specialists, so it is good that Kate Dewar gets her satisfaction from emergency medicine, or that others like to put people to sleep, read slides or x-rays, perform surgery, or see the same diagnoses over and over again in subspecialty practices. But we need a lot more primary care doctors – and nurse practitioners – more family doctors.
We need policies at every level, at those of the medical school and the LCME, and the ACGME, and the state and federal governments, that encourage us to take students who are more likely to enter primary care, to nurture them through their training so that they actually do enter primary care, and to provide a practice setting in which they can feel satisfied that they are providing excellent, patient centered – and population-conscious – care without giving up all of their personal lives.
.
No comments:
Post a Comment